The Divergent Pathways
by Brechtje Sebregts
Ling Shu (Divine Pivot) Chapter 11 is the oldest written source that mentions the divergent pathways (jing bie). Current theories about the use of the divergent pathways are based on interpretations of this chapter and clinical experience. Whilst the Ling Shu only describes the course of the 12 divergent pathways, contemporary authors and teachers have presented their own understandings and methods of treatment. In the experience of this author, the divergent pathways are an effective method for the treatment of chronic complaints. This article introduces the basic theory of the divergent pathways with a detailed presentation of the sixth divergent pair and an illustrative case study. It has been adapted from a chapter of the author’s recently published book Divergent Trajectories – Backgrounds and Applications in Practice.
Introduction
Ling Shu (Divine Pivot) Chapter 11 is the starting point for understanding the divergent pathways. The fact that a whole chapter is devoted to the divergent pathways suggests that this part of the meridian system is important. At the same time, this text raises many questions due to its limited description of these meridians. In the chapter, after a short introduction, Qi Bo describes the divergent pathways in terms of six yin-yang pairs. For each divergent pathway, the region where the pathway branches off from the primary meridian is described, along with the course of the pathway and the region where the pathway re-joins the primary meridian. No further description of function, diagnostic methods, pathology or methodology is described. This has led to considerable variation in the use of the divergent pathways.There has been more innovation in methods of working with the divergent pathways in the past 40 years than in the preceding 22 centuries. Tadashi Irie, Kodo Seki, Shigeji Naomoto, Jeffrey Yuen, Miki Shima, David Twicken and Josef Müller have all contributed to this development. They all describe different methodologies whilst emphasising the clinical relevance of this part of the meridian system. Their understandings are based on years of clinical observation, oral and written transmission from a long tradition of Daoist masters (in the case of Jeffrey Yuen) as well as modern interpretations of classical texts.
Function
Although the Ling Shu does not describe the specific functions of the divergent pathways, some of the sources named above state that they play a role in keeping pathogens away from the zangfu organs. There are different interpretations about how this is done, by the meridian system overall and the divergent pathways in particular. The following description of this process is based on a synthesis of Chapter 56 of the Su Wen(Basic Questions)and Yuen, Twicken and Shima’s interpretations. The divergent pathways have the capacity to store pathogens along their trajectory. This process of storage is known as keeping the pathogen in latency. The pathogen will remain latent until the body can remove it or until latency can no longer be maintained. The preservation of latency depends on the condition of the essences: jing (essence), xue (blood), jin (thin fluids), ye (thick fluids), qi and yang. If the essences are sufficient, the body can store the pathogen and keep it in latency. The patient will not necessarily describe any specific complaints if the pathogen is stored in latency, although this will adversely affect the circulation of qi and blood, gradually restricting physical and mental-emotional movement. For example, a person may become more and more irritable, or start to notice restricted range of motion in a joint. If there is free circulation of qi and blood, then the body may be able to remove the pathogen itself. However, if the essences decrease, the body will no longer be able to store the pathogen and the patient will experience symptoms as the body attempts to eliminate it. This results in chronicand intermittent complaints that vary in frequency and intensity. Such pathology is a specific indication for the use of divergent pathways in treatment. The divergent pathways are therefore indicated for chronic musculoskeletal pain, chronic diseases of the skin and the sense orifices (eyes, ears, nose and mouth), chronic organ diseases and chronic mental-emotional problems. Asking about a patient’s complaints is one of the primary diagnostic methods for determining whether there is a pathogen in the divergent pathways. The 12 divergent pathways are distinguished according to the specific physical and mental-emotional complaints that occur when a pathogen is located in a given pathway. In this article the specific indications for the Large Intestine and Lung divergent pathways are presented, along with points and a treatment method for the Large Intestine.
Indications
Included below is a description of the sixth divergent pair: the Large Intestine and the Lung, including an overview of the physical and mental-emotional complaints related to this pair and a treatment protocol for the Large Intestine divergent pathway. Before treatment it is important to determine whether there is any deficiency in the essences that may be preventing the pathogen from being stored or removed. If so, tonify these essences before undertaking the first step in the protocol. If there is no deficiency, immediately begin with the first step. A case study is included to illustrate how the divergent pathways can be applied in practice.This pair of divergent pathways can be used to treat complaints related to the Large Intestine fu, Lung zang or problems along the course of these pathways. Some of the complaints associated with the divergent pathway of the Large Intestine overlap with those of the Lung. This is because they form a pair. In the vast majority of cases, the complaints are chronic and periods of exacerbation alternate with periods of remission. No clear pattern is discernable in terms of the duration of these phases.
Physical indications
Large Intestine
• complaints along the course of the pathway: stiffness, pain, immobility, weakness or numbness of the shoulder and arm
• chronic pathologies of the Large Intestine and Lung including:
– respiratory complaints: cough, wheezing, shortness of breath or chest pain
– digestive complaints involving diarrhoea, borborygmi, constipation or abdominal pain
– skin complaints accompanied by itching, redness, dry or scaly skin
– throat-related symptoms: swollen throat, sore throat, difficulty swallowing, hoarseness, rattling in the throat, swollen lymph nodes
– pathologies involving the nose: stuffy nose, persistent runny nose, sneezing and itching of the nose
Lung
• complaints along the course of the pathway: pain of the upper arm, shoulder and/or elbow, limited range of motion of the arm, and difficulty opening the hand
• chronic pathologies of the Lung and Large Intestine including:
– respiratory complaints: coughing, coughing up phlegm or blood, shortness of breath or wheezing, chest pain, oedema in the lungs
– excessive sweating, oedema of the limbs, dry skin, dry mucous membranes
– throat-related symptoms: swollen throat, sore throat, difficulty swallowing, hoarseness, rattling in the throat, swollen lymph nodes
– pathologies of the nose: nosebleeds
Mental-emotional indications
Mental-emotional complaints involving the divergent pathways of the Large Intestine and Lung involve grief (bei) and worry (you). In the course of everyday life, people experience loss. The extent of this loss varies, from minor loss of belongings to major loss of loved ones. When a person is in balance, they can accept such loss and let go. Grief is a normal response to loss. It is usually caused by an unpleasant, painful or disappointing situation of loss, or by drastic changes to daily routines and ways of life that have provided comfort, security and stability. Grief can take many forms, including sadness and heartbreak. It is the price that we must pay for being able to love. Sometimes grief is experienced as being traumatic, and can be difficult to resolve. The patient may not be able to process the griefdespite the passage of time. If the patient is overwhelmed by grief, they may not know what to do anymore or not havethe strength or the will to act. Their qi disappears, leaving avoid.
In the words of the Su Wen:
When one is sad, then the heart connection is tense.
The lobes of the lung spread open and rise and the upper burner is impassable.
The camp [qi] and the guard [qi] do not disperse.
Heart qi is in the center.
Hence, the qi dissipates.
– Unschuld & Tessenow, 2011, p. 595
Worry (you) also affects the Lung and Large Intestine. Worrying is a form of thinking about the future in a way that makes the patient anxious or concerned. It is contrary to the movement of life. The term ‘you’ implies oppression, a lack of circulation, contraction and immobilisation. The top of the character you contains the head, the middle contains the Heart and the bottom contains the trailing legs. Thus, the patient lives with problems in the head and the Heart. Qi slows down, and Lung qi stagnates.If the patient cannot stop worrying or is stuck in their grief process, they can be withdrawn and gloomy. They may maintain a happy exterior in an effort to convince themselves and others that everything is okay. Privately, however, they may be consumed with grief. Sadness and grief directly affect the centre of vitality.
Chapter 8 of the Ling Shu states:
In the state of sadness and affliction (bei ai) one is moved to the centre, there is a drying up and interruption and life is lost.
– Larre & Rochat de la Vallée, 2005, p. 125
The divergent pathways of the Large Intestine and Lung should be considered when patients are affected by these emotional states.
The divergent pathway of the Large Intestine
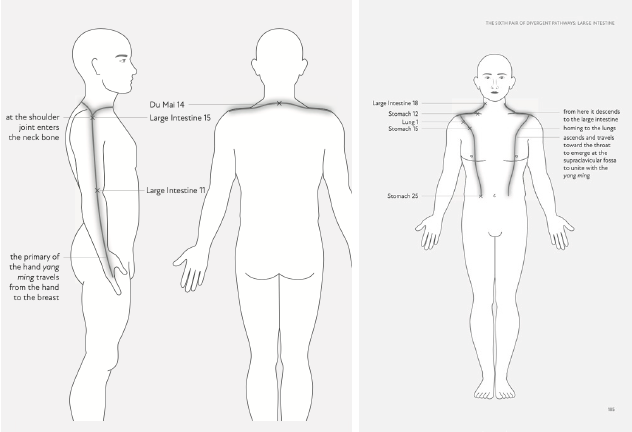
Chapter 11 of the Ling Shu describes the course of the divergent pathway of the Large Intestine as follows:
The primary of the hand yang ming travels from the hand to the breast. A divergence at the shoulder joint enters the neck bone. From here it descends to the large intestine, homing to the lungs. It then ascends and travels toward the throat to emerge at the supraclavicular fossa to unite with the yangming.
-Chace & Shima, 2005, p. 30
Acupuncture points
The Ling Shu describes the regions where the divergent pathways begin and end. In order to treat the divergent pathways, acupuncture points are chosen in these zones. These points are known as the confluence points. The lower confluence point is the start of the divergent pathway and the upper confluence point is its end point.
Lower confluence point: Quchi LI-11
Upper confluence point: Futu LI-18
In addition to the confluence points, Yuen and Twicken include trajectory points in their divergent pathway treatments. These are primary meridian points that lie along the course of the divergent pathways and that are suitable for pathologies of these pathways. Given the general way that the pathways’ courses are described, it is not surprising that a variety of trajectory points have emerged. The selections here remain faithful to the Ling Shu descriptions. It is only necessary to add one or two trajectory points to divergent pathway treatments to make treatment more effective. Decide which of the following points are the most appropriate of the divergent pathway by correlating their functions with the patient’s physical or mental-emotional complaints. They can be needled unilaterally according to the location of the complaint.
Jianyu LI-15 (Shoulder Bone)
Due to its location, Jianyu LI-15 is often used as a trajectory point for shoulder and arm complaints such as stiffness, pain, immobility, weakness of the shoulder and numbness in the upper arm. It promotes movement of qi and blood in the upper arm and shoulder. This restriction of movement with pain is analogous to being stuck in grief or loss. In such cases, Jianyu LI-15 can help a person let go of the past.
Dazhui DU-14 (Great Hammer)
As a trajectory point of the divergent pathway of the Large Intestine, Dazhui DU-14 is not used to treat physical complaints. For mental-emotional complaints, the point can be used when the patient is stuck or experiences persistent negative emotions (e.g. they feel gloomy or depressed and have started to behave accordingly). The patient may no longer spend time with others or engage in fun activities because they do not derive enjoyment from them. DazhuiDU-14 can be used to break these behavioural patterns. The goal is for the patient to re-engage, see people again and discover that life has much to offer.
Zhongfu LU-1 (Middle Palace)
Zhongfu LU-1 makes qi descend and clears the chest in cases of coughing, shortness of breath, coughing blood and pus, wheezing and chest pain. Persistent sadness may also obstruct the descending movement of qi. Shallow breathing or feeling short of breath may indicate that the patient is unable to let go if there is grief and loss. As a result, there is no room to let in anything new. Sadness can lead the patient to no longer make new contacts because they are aware that there is much to lose. Zhongfu LU-1 softens this feeling of isolation and alleviates sadness that has persisted for too long. The patient’s chest feels free and their breathing becomes normal again; they can take theirfirst steps towards processing their grief.
Wuyi ST-15 (Room Screen)
This point is used to treat physical complaints of the Lung. It allows rebellious qi to descend and clears the chest to alleviate coughing, wheezing, shortness of breath and chest pain. Pressure on the chest is often felt when there is not enough space for one’s own needs and feelings. Just as a screen divides a room and creates a feeling of privacy, Wuyi ST-15 can offer protection from external stimuli and allow the patient room for their own needs and feelings.
Quepen ST-12 (Empty Basin or Broken Bowl)
Quepen ST-12 is used to resolve stagnation causing shoulder pain that radiates to the neck, upper arm pain, inability to raise the arm and deafness. Quepen ST-12 also allows Lung qi to descend in cases involving chest and upper warmer complaints, including coughing, shortness of breath, fullness in the chest and swollen glands. When palpating this point, practitioners may feel a lack of muscle tone and often perceive a void. In such cases, the ‘bowl’ is broken and life energy is flowing away. Quepen ST-12 can be used to mend the bowl, so that the patient can collect their qi and resume living.
Tianshu ST-25 (Celestial Pillar)
Tianshu ST-25 regulates the qi of the intestines and removes stasis in the lower burner. It can be used for complaints such as diarrhoea, borborygmi, constipation and abdominal pain. A pillar provides strength and a solid foundation. Thus, this point provides the patient with a stable centre in case of excessive worry. This prevents the patient from losing their grounding. From a stable centre, they can orientate themselves and continue along their life path.
Treatment plan
The following step-by-step treatment plan was inspired by the theories and methods of Seki, Shima, Helms, Yuen, Twicken and Müller. The order of the steps is important.
Step 1: Needle the lower confluence point Quchi LI-11 on the left, then on the right. Then, repeat the process for the upper confluence point Futu LI-18, first on the left, then on the right.
Step 2: Use one or two appropriate trajectory points for the pathology being treated. Select the point(s) based on the location of the complaint, palpation of the trajectory points and information gleaned from talking with the patient. In this way, the trajectory point(s) corresponding to the patient’s current needs can be determined.
Step 3: If the pulse becomes tight at the superficial level in a given position during the treatment of the divergent pathway, needle the jing-well point Shangyang LI-1.
Case study
When Cathy, aged 54, entered my clinic, I noticed that she had considerable redness on her face, especially beside her nostrils. She said that it was not only the skin on her face that was red and chapped. She pulled up her sleeve and showed me a large, similarly red and dry spot on her right wrist, around Yangxi LI-5. She told me that there were periods when her skin issues had been less severe. Cathy did not know what caused her skin to worsen. After some thought, she mentioned her work. She had been self-employed for four years and worked alongside two other women. Their working relationship was turbulent. ‘That’s how it goes, unfortunately,’ she said. It was not only Cathy’s skin that was bothering her. Her nasal passages were full of mucus, sometimes for days at a time, sometimes for several weeks. In addition, Cathy had been constipated for several months. Every four to five days she passed strong-smelling stools; this had occurred at other periods in her life.
I used a combination of four diagnostic methods: asking about complaints, pulse diagnosis, abdominal diagnosis and kinesiological testing. Based on the location and the chronic and intermittent nature of her symptoms, I determined that Cathy’s complaints involved a pathogen in the divergent pathway of the Large Intestine. I also diagnosed deficiency of qi, which was preventing her body from holding the pathogen in latency.
I first needled Qihai REN-6 to tonify qi, and the mu point of the Large Intestine, Tianshu ST-25, to move qi in the colon. In the same treatment, I added the divergent pathway of the Large Intestine.
First, I needled the two lower confluence points: Quchi LI-11 on the left and on the right. Then, I needed the two upper confluence points: Futu LI-18 on the left and then on the right.I did not use trajectory points of the pathway of the Large Intestine in this treatment, as they would not have added anything for the treatment of her complaints. Locally, I used Yingxiang LI-20to relieve Cathy’s congested nose. I explained at the end of the treatment how she could massage Hegu LI-4 herself. J.R. Worsley nicknamed this point ‘the great eliminator’ because of its powerful clearing effect on blockages of the Large Intestine, which removes toxins and other waste. In treatment of the divergent pathways, diagnostic methods act as a feedback mechanism. Improvements in, for example, pulse or hara indicate a positive treatment outcome. So 10-20 minutes would be allowed to elapse before noticing signs of improvement. As soon as no further improvements are observed, the needles can be removed. In the vast majority of cases, instantaneous improvement in the patient’s complaints should not be expected; in some cases, however, these are immediately observable. In most cases, a gradual reduction of symptoms occurs, which usually manifests itself in the days following a treatment. The changes reflect a general improvement in the patient’s functioning and in specific aspects of the meridians and organs (zangfu).
Two weeks later, I saw Cathy again. Her bowel movements had improved: she was now passing stools every two days that did not smell much anymore. The conversation turned to the red and dry spots on her skin, which were still evident. I explained that the redness and heat that she experienced had to do with waste and toxins in her body. An appropriate metaphor would be a full rubbish bin that cannot be emptied. As a result, the bin stinks and the rubbish rots. Cathy’s constipation was the physical manifestation of that full bin. I cautiously brought up the topic of work. Cathy admitted that she clung to the past in the form of people or objects that she could not let go of to make way for something new. She knew that this situation was not healthy for her. Cathy said that letting go was difficult for her as this would lead to a change in who she was, which was scary. This prevented her from seeing new possibilities and new sources of inspiration.
I started the next treatment by opening the Du Mai Governing Vessel), Houxi SI-3 on the right and Shenmai BL-62 on the left. This would help Cathy stand on her own feet with a straight back and show who she was and what she wanted. Full of yang, the Du Mai could give her life movement and firmness. I combined the Du Mai with the divergent pathway of the Large Intestine. I needled the lower and upper confluence points first and then added Dazhui DU-14 as a trajectory point, to enable Cathy to consider the possibility of working with other people. I added Tianshu ST-25 to provide Cathy with a stable centre from which to break down the calcified patterns and relationships, enabling her to grow and develop. In the four treatments that followed, I kept tonifying her qi and stimulating movement in the Large Intestine, both physically and mentally. In the seventh treatment, I diagnosed that she had sufficient essences and I used the divergent pathway of the Large Intestine again to support the body in getting rid of the pathogen which was located within it.
At the following treatment, the redness on her face and right wrist was barely visible and the constipation had improved. Based on the four diagnostic methods, I determined there no longer was a pathogen in the divergent pathway of the Large Intestine. Cathy told me how she was dealing with her situation at work. She talked to her colleagues and shared her qualms about their working relationship. She indicated that she would look for another job and that she did not want to continue as she had before.
The rhythm and peristaltic movement of clearing and letting go had returned.
This article was first published by the Journal of Chinese Medicine | Issue 128 | February 2022 and is republished with permission.
Bibliography:
- Cecil-Sterman, A. (2012).Advanced Acupuncture. A Clinical Manual. First edition. Classical Wellness Press: New YorkChace, C., Blalack, J. & Schaefer, J. (2007). Lurking Pathogens: Three modern Approaches.The Lantern, 4, 2-3, pp. 17-27, pp. 40-45
- Chace, C. & Blalack, B. (2006). Lurking Pathogens: A Case Study fromthe late Qing Dynasty.The Lantern, 3, 1-2, 23-37 and 40-45
- Chace, C. (2009). The Merging of Ways, an Approach to Understandingthe Channel Divergences in Meridian Style Therapy.The Lantern, 6-2, 14-21
- Chace, C. & Shima, M. (2011).Exposition on the Eight Extraordinary Vessels: Acupuncture, Alchemy and Herbal Medicine. Eastland Press: Seattle
- Chace, C. (2018). Fantasy Maps and How to Use Them: Rooting Channel Divergence Theory in Palpatory Experience. Journal of Chinese Medicine,118, pp. 5-13
- Deadman, P. & Al-Khafaji, M. (2007).A Manual of Acupuncture. Secondedition. Journal of Chinese Medicine Publications: Hove
- Denmai, S. (2003). Finding Effective Acupuncture Points. EastlandPress: Seattle
- Ellis, A., Wiseman, N. & Boss, K. (2012).Grasping the Wind. ParadigmPublications: Brookline
- Farrell, Y. (2016).Psych-emotional Pain and the Eight Extraordinary Vessels.Singing Dragon: London (UK)
- Hicks, A., Hicks, J. & Mole, P. (2011).Five Element Constitutional Acupuncture. Churchill Livingstone: London
- Jarrett, L.S. (2015).The Clinical Practice of Chinese Medicine. Spirit PathPress: Stockbridge
- Jensen, A.M., Stevens, R. & Burls, A. (2014).Developing the evidence for kinesiology-style manual muscle testing: A series of diagnostic test accuracy studies. Elsevier: London
- Kaatz, D. (2011).Characters of Wisdom – Taoist Tales of the AcupuncturePoints. (E-book) The Petite Bergerie Press
- Larre, C. & Rochat de la Vallée, E. (2003).The Secret Treatise of the Spiritual Orchid. Monkey Press: London
- Larre, C. & Rochat de la Vallée, E. (2005).The Seven Emotions. Monkey Press: London
- Maciocia, G. (2005).The Foundations of Chinese Medicine. Churchill Livingstone: London
- Matsumoto, K. & Birch, S. (1988).Hara Diagnosis: Reflections on the Sea. Paradigm Publications: Brookline, Massachusetts (USA), 387
- Matsumoto, K. & Euler, D. (2012).Kiiko Matsumoto’s Clinical Strategies,Vol.1. David Euler, 299
- Müller, J.V. (2004). Den Geist verwurzeln. Verlag Müller und Steinicke: München
- Müller, J.V. (2018). Den Geist verwurzeln. Band 3. Verlag Müller und Steinicke: München
- Müller, J.V. (2020). Den Geist verwurzeln. Band 4. Verlag Müller und Steinicke: München
- Scheid, V. (2014). Transmitting Chinese Medicine: Changing Perceptionsof Body, Pathology and Treatment in Late Imperial China,Asian Medicine,8(2), 299-360.
- Scheid, V. (2018). Promoting free flow in the networks: Reimagining the body in early modern Suzhou, History of science, 56 (2), 131-16
- Shima, M. & Chace, C. (2001).Channel Divergences: Deeper Pathwaysof the Web. Blue Poppy Press: Boulder
- Solinas, H., Mainville, L. & Auteroche, B. (1998).Atlas of Chinese Acupuncture: Meridians and Collaterals. 3-8-3 Publishing Canada
- Sommers, D. (2007).De Chinese fascinatie voor de geest. Uitgeverij Libra& Libris: Veghel
- Twicken, D. (2014).Divergent Channels – Jing Bie: A Handbook forClinical Practice and Five Shen Nei Dan Inner Meditation. Singing Dragon:London (UK)
- Twicken, D. (2015).The Luo Collaterals: A Handbook for Clinical Practice and Treating Emotions and the Shen and the Six Healing Sounds. SingingDragon: London
- Unschuld, P. (2016).Huang Di Nei Jing Ling Shu: The Ancient Classic on Needle Therapy. University of California Press: Berkeley
- Wang Ju-Yi & Robertson, J. (2008).Applied Channel Theory in Chinese Medicine: Wang Ju-yi’s Lectures on Channel Therapeutics. Eastland Press: Seattle
- Yuen, J.C. (n.d.).The Divergent Channels of Classical Chinese Medicine [DVD]. ACCM